Respiratory Synctial Virus (RSV) is not the Flu. Nor is Covid-19. Both are much like the Flu. At least, they are much more like the Flu than they are like any other major illness category. Within the step-wise decision – guiding protocols of respiratory virus surveillance, the Influenza – like – illness (ILI) category covers RSV, Covid-19, Influenza and more.
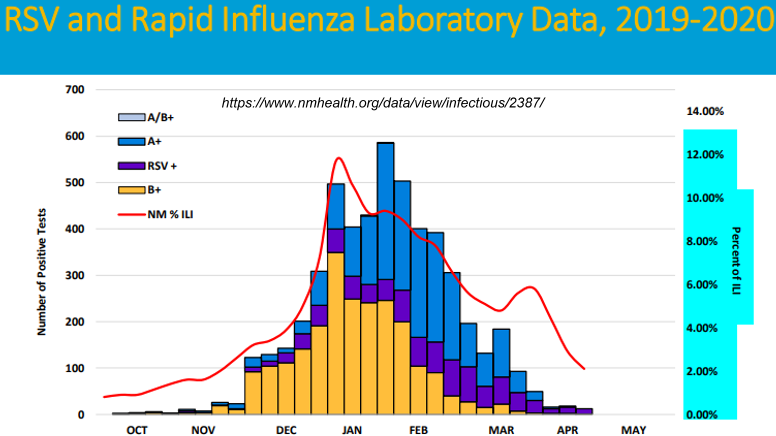
ILI is a fairly special category because it details the numerous decisions that must be made and steps that must be taken, as well as steps that should not be taken (by default, if it circumvents the protocol, it should not be practiced) by health professionals in regard to annual emergence and decline of respiratory fevers. For example, RSV and Influenza data are included in reports by states such as New Mexico and others as they conduct continuous surveillance of Influenza-Like-Illnesses (ILIs). The featured image above explains clearly enough for both.
ILI is also an ecumenical category, or at least it used to be. Depending on the surveilling state (in the US) this surveillance includes a wide variety of virus/illness types, from influenza through RSV, adeno, parainfluenza, rhinitis, and all coronavirus categories with the exception of Covid-19. Here below, from the link in the first sentence of this paragraph, is a nice example of how the CDC’s surveillance covers the other coronaviruses that are closely related to Covid-19.
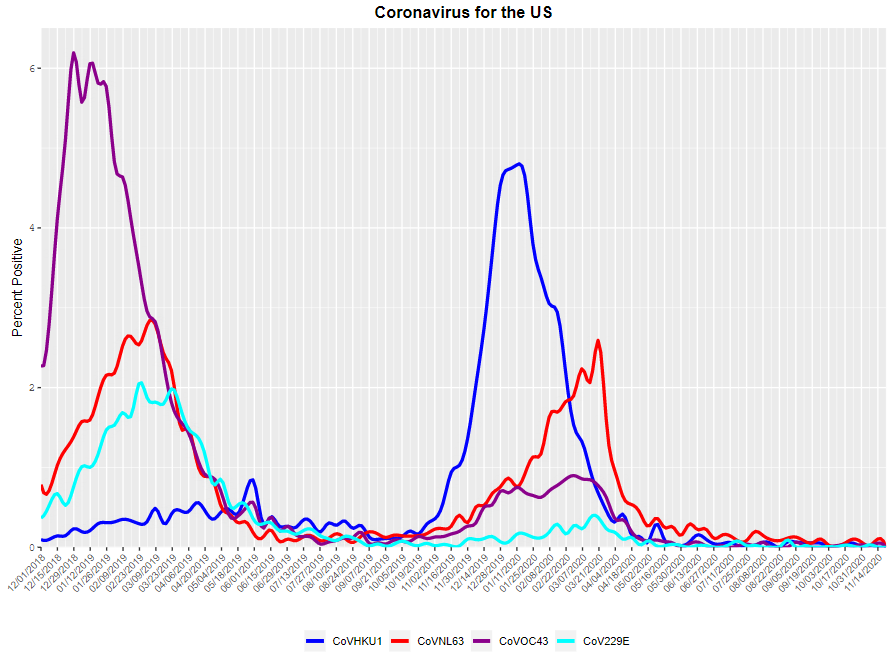
All of the standard coronavirus cases appear to be seasonal and are monitored based on illness.
I note also, even though the CDC will not, that the apparent seasonality of coronavirus illnesses is much like the seasonality of flu virus cases.
Each of the charts above are derived ultimately from patients. These charts therefore build the otherwise obvious case that the mass testing of people who are not ill, for only one respiratory virus, is not surveillance. Not to overstate but again the standard respiratory illness surveillance derives from people who were ill that were attended to in some medical way, up to and including an appointment with a doctor or equivalent. This surveillance is geared to develop a continuously updated picture of types and varieties of respiratory viral illnesses that circulate through our communities up to and including the national level. Moreover, the only effective means to surveil must include testing across the range of virus illnesses that are known to prevail. The featured chart is an example. RSV is not Influenza or Covid-19, but it can be as serious as either and it clearly is surveilled as an ILI, or at least as a close covariate.
RSV can be tested by antigenic methods for its identification. Antigenic methods typically involve infecting ferrets or rodents with the candidate virus strains in order to harvest the resulting antibodies. Researchers assert that these animals get the same flus as we do. I haven’t checked but I suppose they don’t produce exactly the same responsive antibodies as we do, because the antibodies they produced for us are not used to fight anyone’s illness. They are only applied to a plate of samples from a patient’s mouth or nose. A color change signifies that a notable proportion of the antibodies have paired with the virus’s protein stubs. The illness is accordingly nominally identified.
After the front line antigenic tests, there are also well known genetic tests. As an interesting nanoscience part of those, electrophoretic sedimentation methods (I call them that) are used to disambiguate one virus strain from another. The tests are precise, but outside of a patient-in-a-hospital context, the genetic test doesn’t necessarily tell one much. That’s because we live and breathe in a sea of airborne encapsulated viruses. Every nanosecond, these drift and flow and sometimes lodge within your respiratory freeway on their journey to and from the atmosphere. No need to panic, as your own antibodies keep them in line. Most are encapsulated anyway, so they don’t even trigger an antibody. Any genetic test imaginable cannot know that. So the test will find a virus that is sought after, but it doesn’t have any validity to assign an activity to that virus. Accordingly those tests are saved for the hospital patients. The logic of that is much better for surveillance purposes because at least that hospital population is known to be sick with some form of respiratory virus.

The cool violet hue of airborne viruses (and other microbes) swarming over Africa. From [1]
In the branch of surveillance that applies to RSV, antigenic testing is conducted for one type, as the chart shows. This testing is initiated from a standard visit to a physician. And clearly the chart explicitly recognizes, again, that RSVs are a type of ILI.
I think that RSV is somewhat challenging to distinguish from many common coronaviruses. They are roughly the same size and shape. And they both have glycoprotein stubs, which are the business ends that allow infection. And so on. But at least RSV can be differentiated from Flu through antigens. And, given that RSV is included within the CDC’s umbrella of respiratory illness surveillance known as the Right Size Roadmap (RSR), it seems critical and only fair that Covid-19 illnesses should also be included.
Yet currently all Covid-19 illnesses are split off from the RSR surveillance program. That appears to cover about half, if not more, of what the RSR previously used to regulate. This apparent divergence from the RSR plays out even in the best of RSR-following states. Below is an example from the Iowa branch. They admirably provide a chart showing flu-like cases including RSV, rhinovirus, parainfluenza viruses, adenoviruses, and coronavirus cases, all genetically and/or antigenically validated.
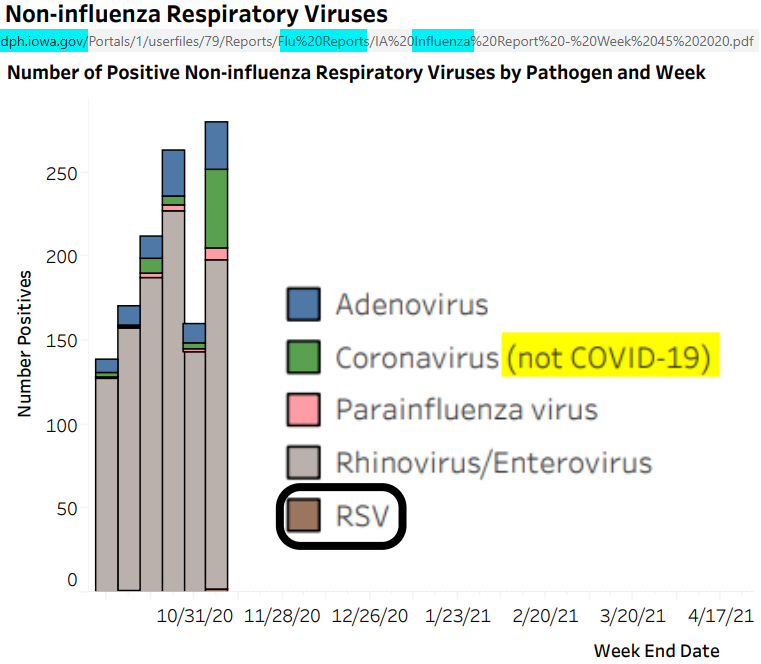
Covid-19 is testable. Yet as with all of their fellow states, SARS-CoV-2 (Covid-19) has been separated from this monitoring stream and diverted to a new, parallel reporting system featured in COVID-NET and COVIDVIEW. As a result, no matter how helpful the Iowa chart may seem, it is not, without the Covid-19 data incorporated. Also, the new COVID surveillance paradigm comingles the patient population with overwhelming numbers of tests from those who are not sick.
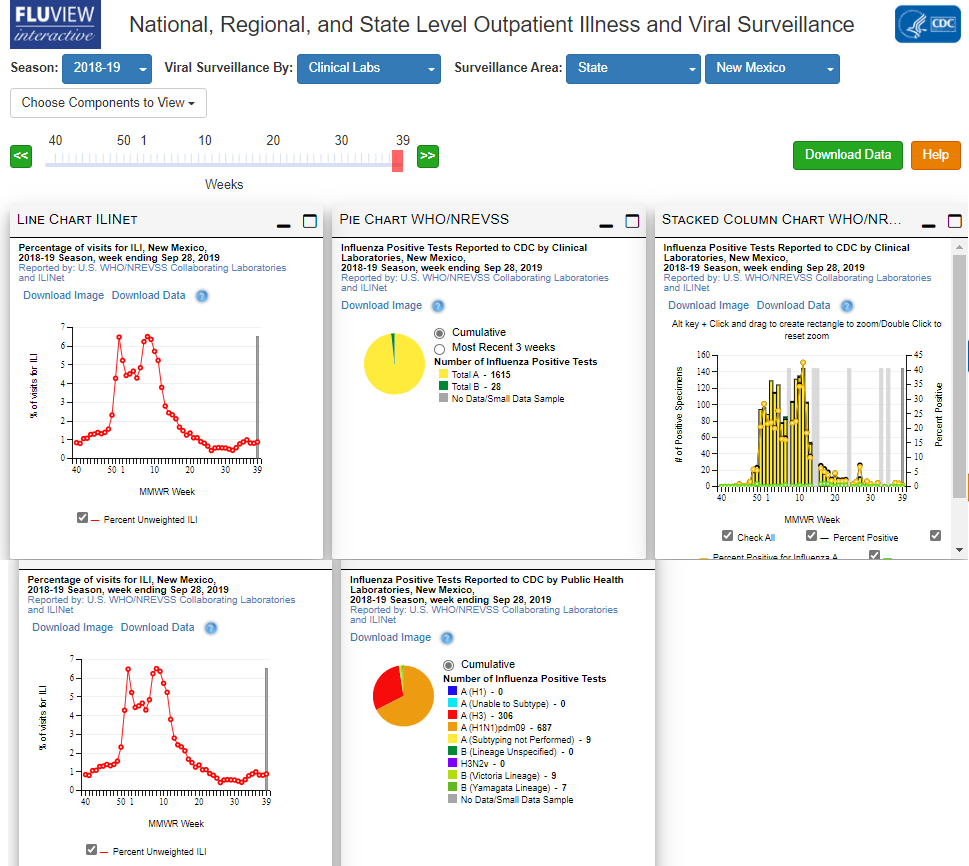
Perhaps due to this comingling, unlike the RSR- aligned FLUVIEW and FLUSurv-NET, the COVID-NET and COVIDVIEW systems do not allow for confirmation or mapping of any antigenic or genetic test. Here is an example of a FLUVIEW interactive report composite for both antigenic and genetic testing. Note that I’ve drilled down from National to Region 6 to New Mexico. The season is 2018 and the two red curves are identical because they cover the same parameter, ILI activity for that year in that state. ILI activity is simply the act of going to an urgent care center or other clinical resource because of a respiratory ailment that is Flu-like. To determine a little more clearly how Flu-like your illness is, the doctor or equivalent is likely to order that simple antigenic test (this is usually the “clinical” category below). The top row of this image below covers such tests. Antigenic tests can identify a few major categories of Flu but they don’t split hairs too finely.
The RSR protocols ensure that the CDC reports laboratory test results associated with flu activity and hospitalizations
Should your Flu-like illness get worse, you may need hospitalization, In that event, doctors are expected to order the second row of tests in the figure above; the genetic tests (typically captured purely by the “public health laboratory” category in the bottom row of the figure). In this genetic laboratory test exercise, they are somewhat more likely to narrow down the specific strain of Flu, if that is what you have.
In conducting this second level of tests, the information may not help them treat you any more effectively than the great care you are probably already getting at that hospital. But it does help them understand what is “going around”, and that is expected to help focus on the best strains to develop vaccines for on the next flu season. That again is the very mission of surveillance.
As a result of that goal, they are expected to report the test result. They must test to determine what you have, and they must report, to help protect people for the next year. If they do not test, and/or if they do not comprehensively report, they would seem to violate the protocol.
In comparison to the Flu test reports above, here is an example of my search for equivalent information from the COVID-NET and COVIDVIEW reports. As this appears to demonstrate, no matter where one searches, the breakdown of antigenic and genetic tests which are supposed to be disclosed are nowhere to be found. Nothing on tests at COVID-NET first:

Nothing in COVIDVIEW either , but that page does have an interesting dataset, which I’ve compiled and charted here:
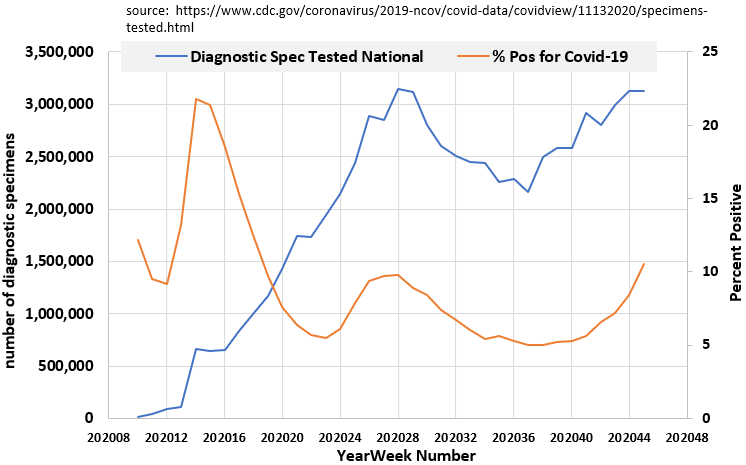
As a departure from the RSR, CDC’s COVIDVIEW does not identify individual states of the US for this laboratory test coverage. Nor does it discriminate between commercial, clinical, or public testing labs, or the types of tests. No mapping is provided for comparison to tests for other respiratory virus types. Antigenic tests if any, might not be included. Anyone who has tried to read through the CDC’s requirements to use antigenic tests for Covid-19 would understand why I suggest this.
Is your brain cramped up by now? The best is yet to come. After all is said and done, it seems apparent that the underlying laboratory genetic test data sets are no longer tethered to actual illnesses. The chart likely includes positive tests associated with at least some of the hospitalizations that would normally trigger such a test. But the sum of millions of specimens collected dwarfs the number of test specimens collected for surveillance of all combined respiratory viruses over any year. If one didn’t know that the RSR protocol was not followed, one might incorrectly conclude that the chart indicated that more than half of all respiratory viral Activity and Hospitalizations should be attributed to something(s) other than Covid-19. The truth again is that most of the tests are no longer tethered to any hospitalization record. This comingling of patient and non-patient testing is not found in normal flu surveillance.
Perhaps that relates to the CDC’s differing guidance for Covid-19 data. Unlike the RSR mandate for influenza, the confirmation of a clinician’s Covid-19 diagnosis is optional:
| https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/purpose-methods.html |
| Testing is performed at the discretion of health care provider |
Moreover, and probably as a direct result, health care professionals cannot so far publicly assure any that the two streams of Covid-19 data and Influenza – Like- Illness (ILI) data are mutually exclusive. Perhaps they can and will some day. But without the confidence of mutually exclusive populations, nothing regarding Covid-19 activities (visits to clinics) or Covid-19 hospitalizations can be taken at face value.
I cannot seem to emphasize enough that genetic tests for Covid-19 are routinely and widely reported for the health. And yet, those ill with respiratory symptoms might never actually be tested for Covid-19, even though the doctor may diagnose them with that.
This is only a blog and only my opinion, and it’s disturbing to any to explore this when lives are in the balance. But at times like these, the candid, mutually exclusive laboratory test information, covering the standard array of respiratory viral candidates, for people who are actually ill, under the accepted RSR surveillance protocol, are more important than ever.
Let’s return all respiratory viral surveillance to the Right Size Roadmap without further delay, and then confidence can be restored eventually. If the tests can confirm something beyond what we normally accept for Flu morbidity, then that is one thing. If the tests/diagnoses are not mutually exclusive from Flu or the other respiratory viral candidates, that is another.
Recommended posts and links:
ALSO
Spike Proteins of Influenza versus Covid-19
Additional source pages. The final site surprisingly is only about ILI:
https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
https://gis.cdc.gov/grasp/COVIDNet/COVID19_3.html
https://gis.cdc.gov/grasp/COVIDNet/COVID19_5.html
https://gis.cdc.gov/grasp/COVIDNet/COVID19_1.html
REFERENCES
[1] Smith, D.J. 2013. Microbes in the Upper Atmosphere and Unique Opportunities for Astrobiology Research. ASTROBIOLOGY. Volume 13, Number 10
 6917total visits,2visits today
6917total visits,2visits today