I’m not any kind of health expert. I only assume that when a physician diagnoses a serious condition, such as cancer, they are expected to verify with one or more diagnostic tests. I gather that these tests are first and foremost for the patient’s protection. There is an apparent secondary benefit to the health care provider. Namely such tests document that the providers practiced due diligence. In other words, they were not negligent, because they didn’t purely rely on subjective judgment.
Why would testing requirements be any different in regard to a diagnosis of Covid-19? They wouldn’t. That’s apparently why for our protection, the CDC and all State health departments followed the Right Size Roadmap (RSR) for sequential testing steps to annually monitor virus strains that infect our respiratory systems. Such strains include influenza, adenovirus, respiratory synctial virus, and yes, several strains of coronavirus. Yet in the Spring of 2020, when the NM DOH, along with most if not all other State health departments, reported almost zero positive results of PCR and/or antigenic tests for the usual strains of Seasonal Respiratory Viruses (SRVs), they may have fallen short of our public respiratory surveillance standards and objectives.
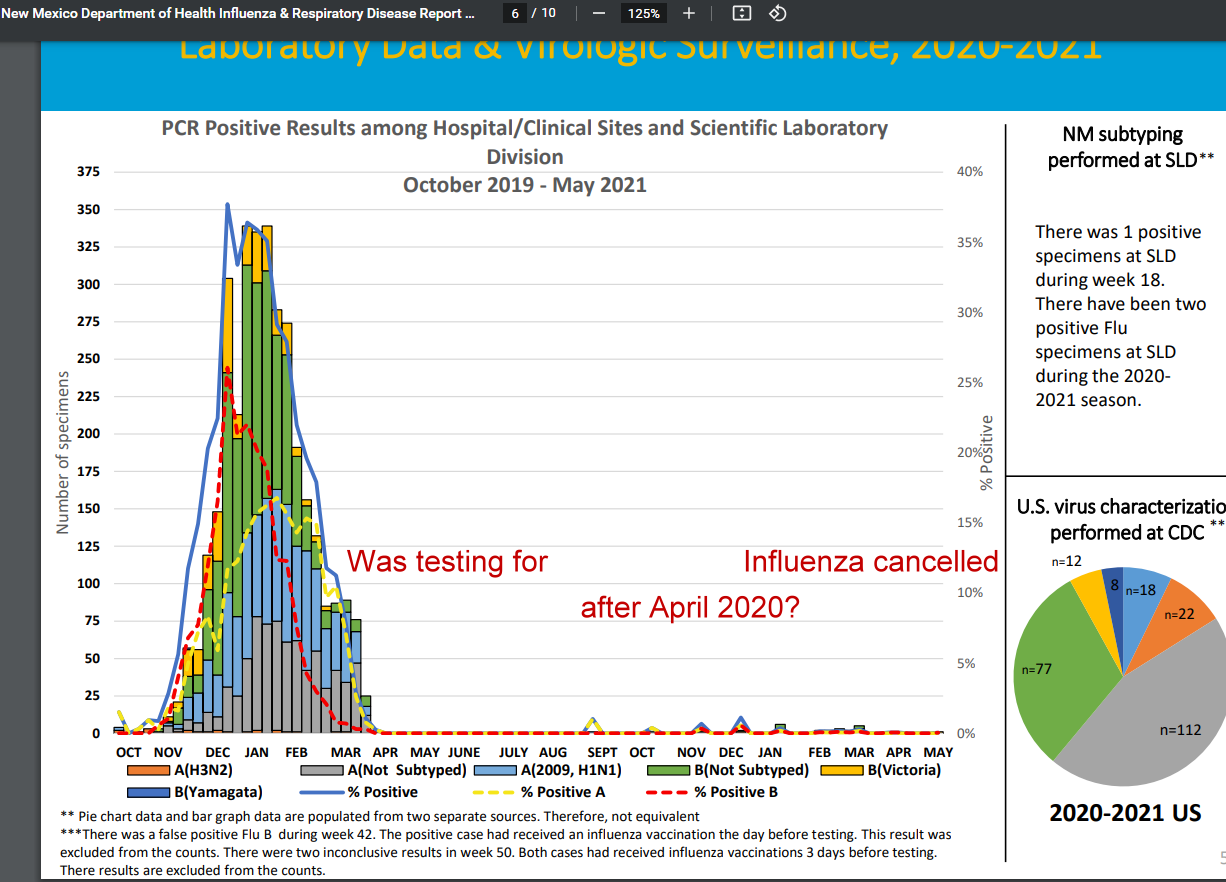
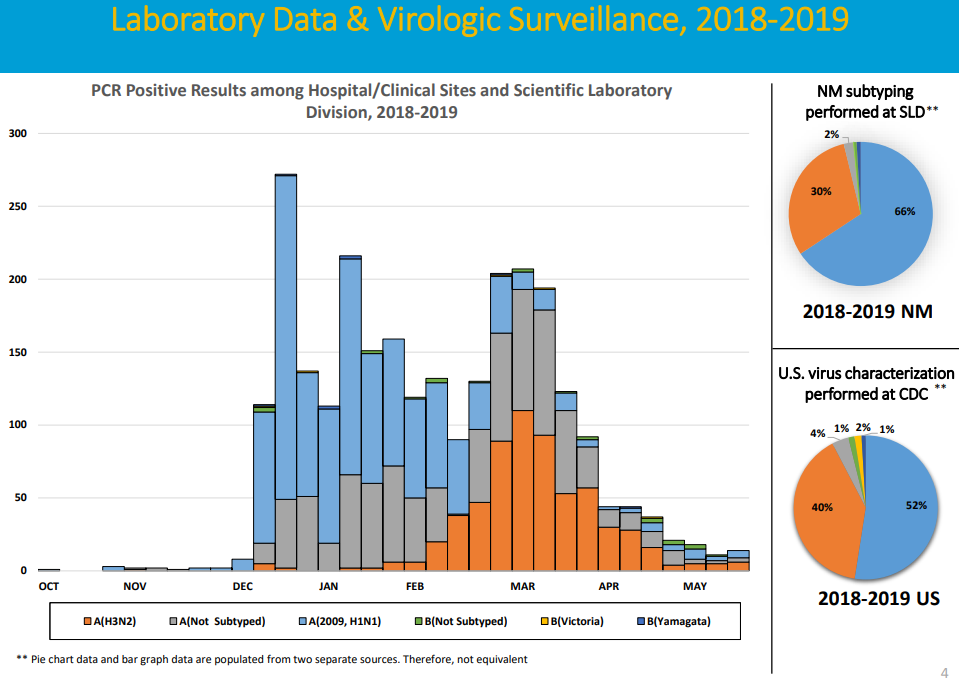
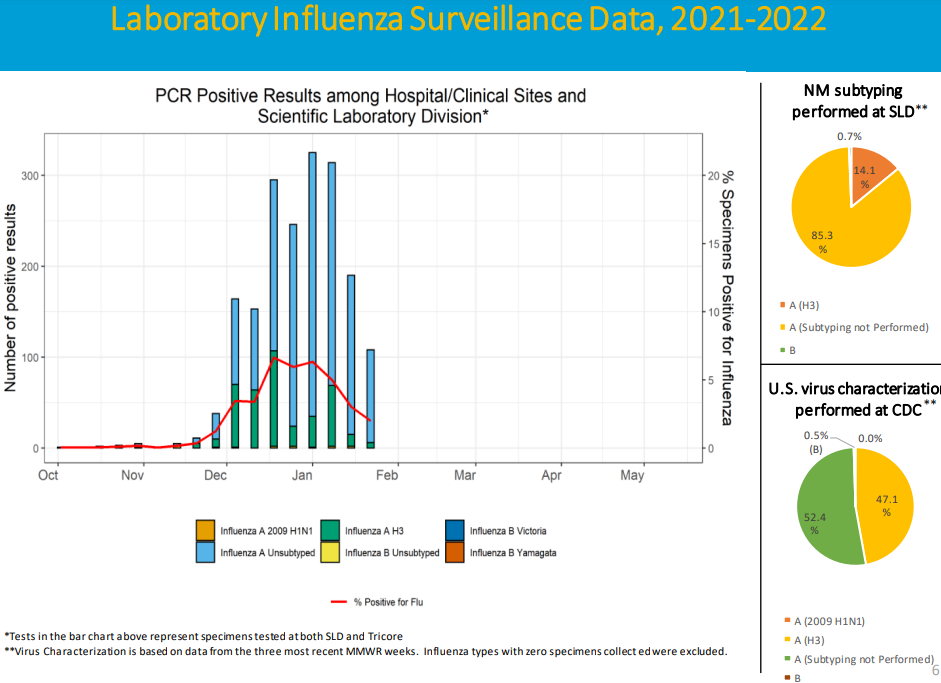
You can confirm that this happened in 2020 and 2021 from the featured image. Our flu season always starts at the beginning of October and ends in May. The stacked bar chart shows on the left that for most of the 2019-2020 season, the NMDOH did surveil many of the typical flu species. And as a paper I coauthored [1] noted, their national partner, the CDC, also counted 4 subtypes of Coronavirus. But after April of that season, and for more than a year beyond, almost no positive tests were reported.
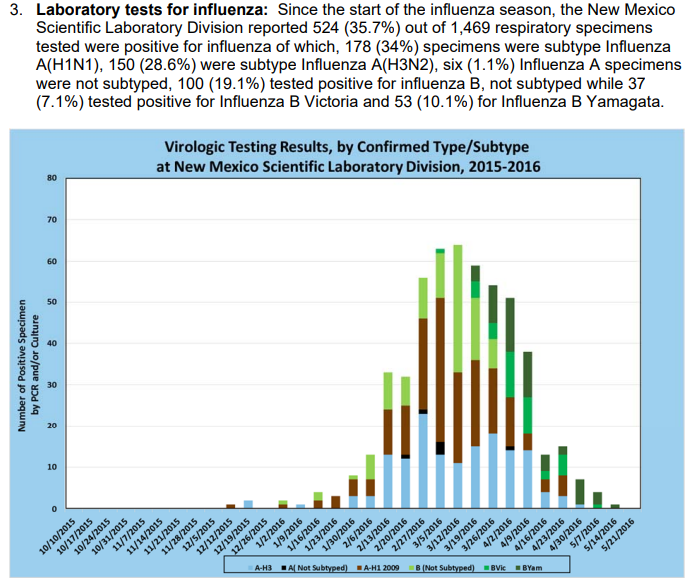
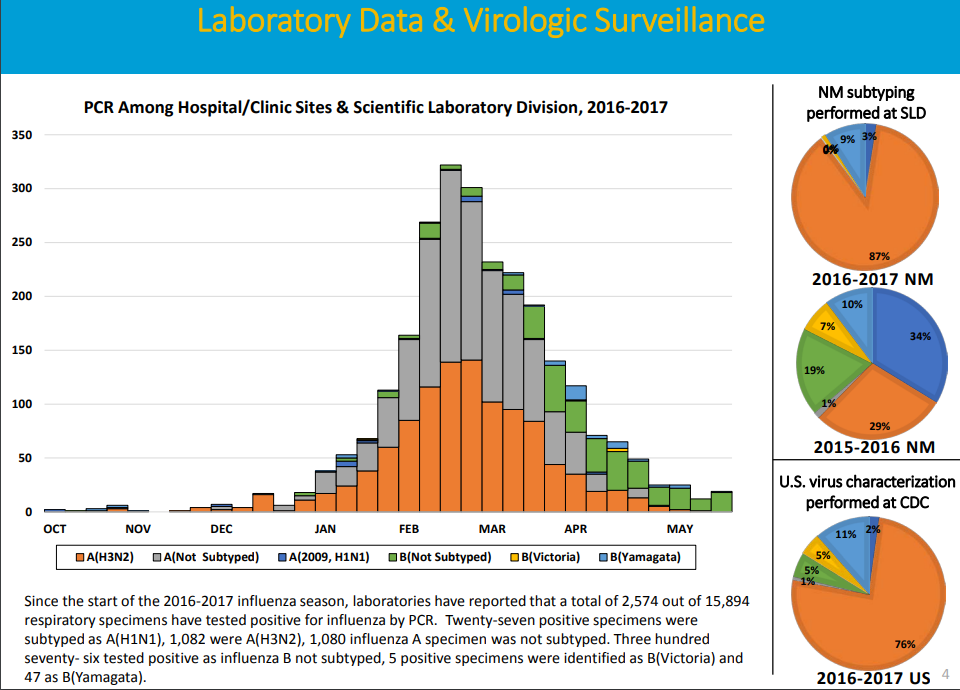
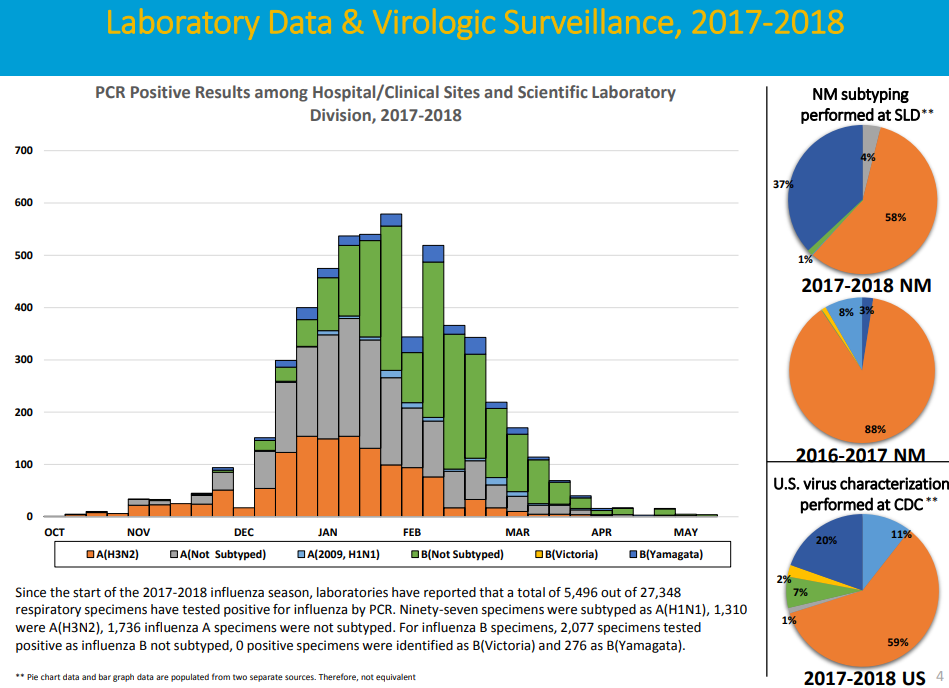
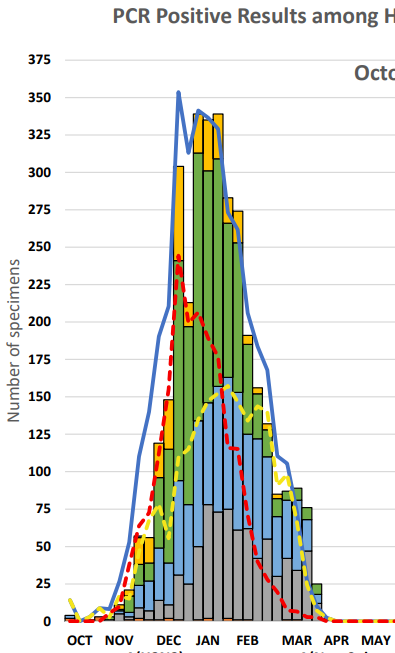
Anyone can visit their pages of reports at https://www.nmhealth.org/about/erd/ideb/isp/data/ going back many years, and confirm that every year, over the flu season, the testing was carried out and the substantial results were reported. To demonstrate, here are the previous test records going back to 2015:
The 2019 – 2020 graph is shown of course at the top of this post. It’s unusual also because it has been stretched out to cover into 2021. Here’s my clip to make it align with the above sets:
Then by April of 2020, the reporting of positive tests appears to have come to an abrupt halt, and didn’t return until this past September of 2021. That accounts for the vast blank area of the next chart.
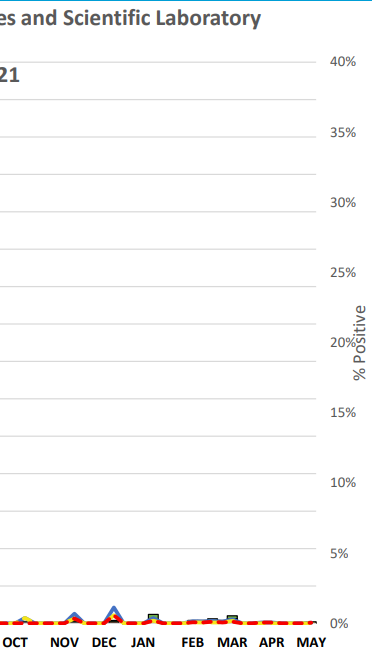
Obviously, this testing gap coincided with the bulk period of the pandemic. Again, over the peak of the pandemic, positive tests of the sick for most strains apparently cannot be found in the normal documentation for respiratory illnesses. There are a few positive tests scattered across the months after April 2020, as the above image shows. Perhaps many tests were actually taken but they were all negative. If you believe that, then you’ll believe this slide I developed from the CDC’s FluView Interactive site.
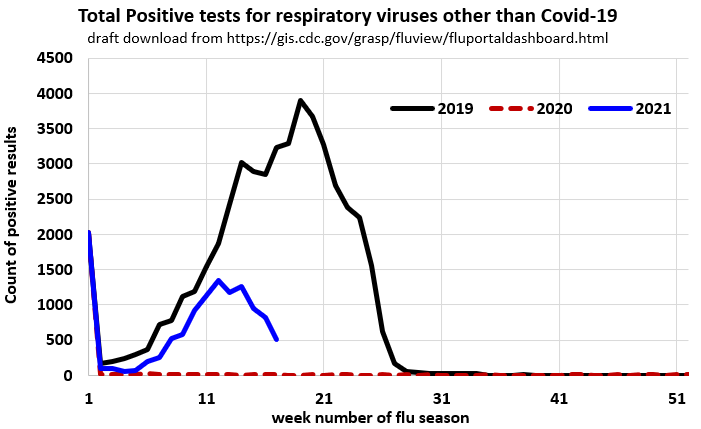
I’ve only profiled a few years but again, all years of surveillance show rough “bell curves” except for the red pandemic year. This pandemic period test record accordingly seems exemplary of an anomaly in scientific circles. One would like to get to the bottom of it, yet no physician or other health official or lawmaker of either party appears to be curious. I’ll go with a null hypothesis until then, that many flu strains were circulating, as they do every year.
From that perspective, the charts above suggest that almost all reporting of positive testing of the ill for expected respiratory virus candidates was halted for a year, even though many tests were submitted. This seems to be corroborated by the CDC itself, which is quoted towards the end of reference [1]:
“Due to the impact of COVID-19 on ILI surveillance, and the fact that the state and territorial epidemiologists report relies heavily on ILI activity, reporting for this system will be suspended for the 2020–21 influenza season”
Accordingly, when surveillance was needed more than ever, it was cancelled, without any concerns raised, except here. The next two charts appear to further support, because they demonstrate that sick people were diagnosed with Covid-19 over the same period that the necessary reporting of the testing featured above, was eliminated. Accordingly, these charts tabulate New Mexico ED (emergency visit) outcomes for Influenza-like-Illness (ILI) and Covid-19-like-illnesses (CLI). It’s also interesting that they have replaced the previous menagerie of virus species with only two categories: Covid-19 SRV and everything else. Note that ILI therefore might be interpreted to signify every SRV other than Covid-19 in these charts. The first chart I’ve copied from their site covers a period from Feb 2020 (when the Pandemic started here in NM) to slightly more than a year later, ending in April 2021.
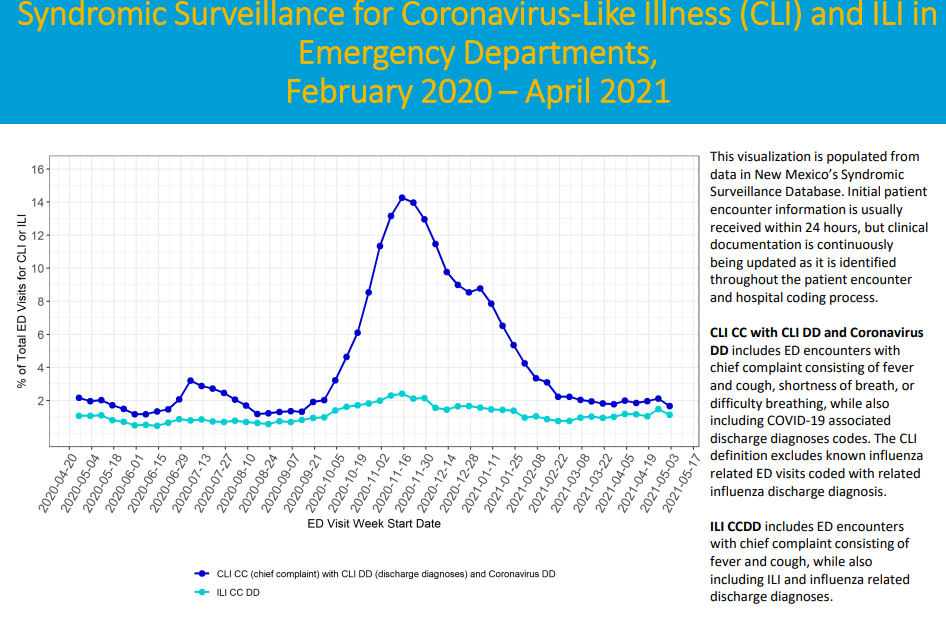
As with the national trend, all reporting of diagnoses for garden variety and typically ubiquitous SRVs dropped to almost nothing, and Covid-19 diagnoses dominated. That’s again historical. Also, the chart does seem to indicate that almost no ED patients were registered for Covid-19 throughout the early half of 2020. That’s also odd because numerous hospitalizations were reported by NMDOH for Covid-19 cases over that period. How did all of those sick Covid-19 sufferers get admitted to those hospitals without showing up on this Emergency Room visit chart? You’d have to ask the hospitals. Here is the second chart of this type:
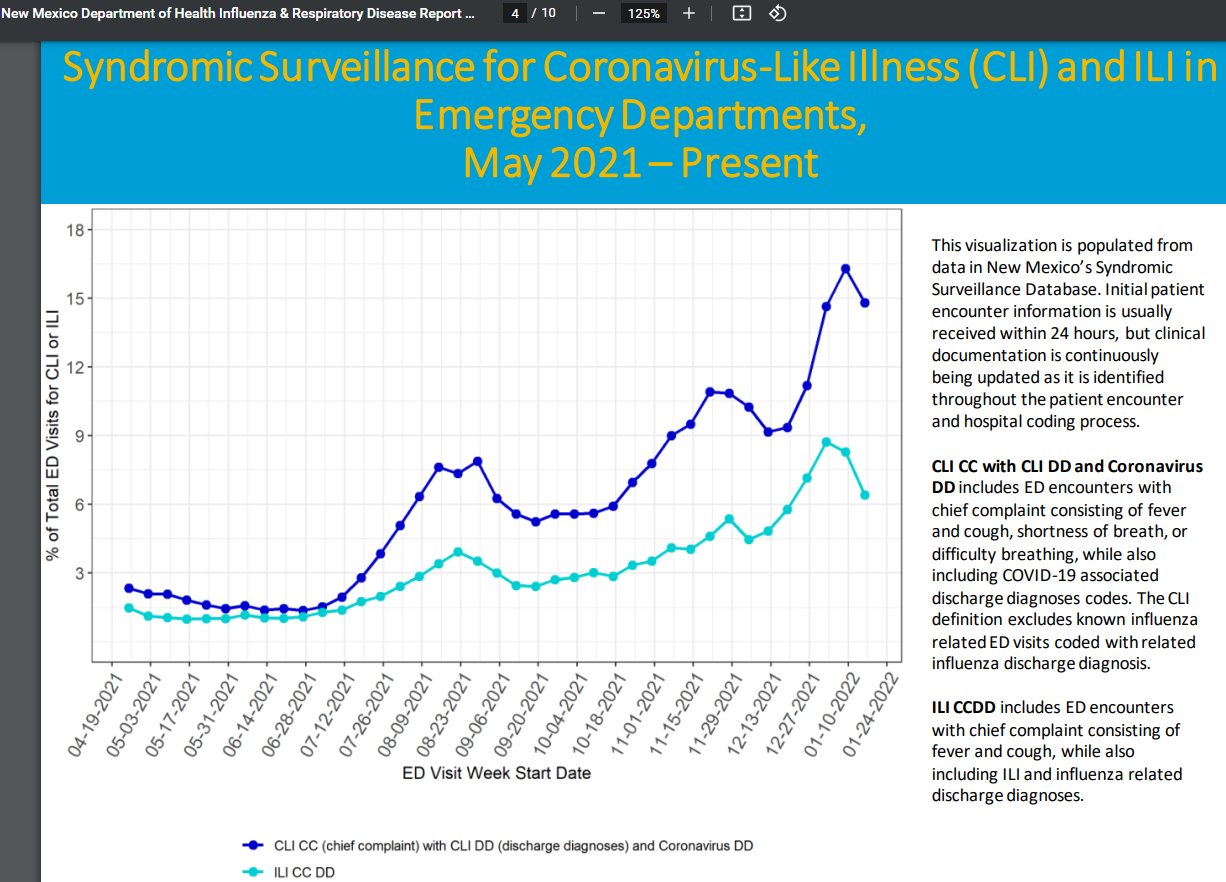
This later chart above is equally interesting. ILI cases account for half of all of the cases now. It’s also notable that CLI and ILI both appear to be back on a seasonal track. I guess that proves that the paper I coauthored {1] was also right about the seasonality of Covid-19. And finally, now some testing is starting to show up again:
Here is a link to that report: https://www.nmhealth.org/data/view/infectious/2615/ But you won’t find any testing documentation concerning Covid-19 there. Only for influenza and RSV. Again these reports suggest they cover all respiratory virus statistics but they don’t report the tests relating to Covid-19 for the sick.
In summary, the information above demonstrates that people were diagnosed with Covid-19 at hospitals and urgent care centers over that same time frame that positive test reporting for the sick dropped to nearly zero. And now, even as influenza testing resumed, Covid-19 tests of patients are not found in these public health documents. It may be that since the CDC cancelled their surveillance without any discussion, and almost no public disclosure, physician opinions are now permitted to tip the scales against antigenic and related testing protocols. Or maybe not. In the RSR-free world of today, without transparent and deeply traceable assurances of mutually exclusive populations of the Covid-19 virus strain SARS-CoV-2 (including its mutating progeny) and the other SRVs, only speculation can follow.
Any might feel free to research into the distinctive signatures/symptoms that someone has Covid-19 and not for example, Influenza of any type. But if they work from the accepted scientific literature, they will come up empty handed. Only a test suite can get one closer to the answer. Reproducible testing under the CDC’s RSR was for all practical purposes, mandated, until it was cancelled. And now that rapid tests are entering the commodity vacuum, things continue to get interesting.
The Syndromic Surveillance charts come with some annotations on the right, but there is nothing stated about tests to validate the conditions of ILI versus CLI. They do suggest that shortness of breath and difficulty breathing are unique to Covid-19. They should write a paper and publish to support that notion, because even the widely believed claim of a unique loss of sense of smell and/or taste is contradicted by papers which note that those are also symptoms found in many influenza patients. Finally, these reports contain an important but odd disclaimer statement on their first page:
“Based on testing results, we interpret ILI currently in NM as primarily a reflection of COVID-19 activity, with moderate influenza and RSV activity.”
I interpret this to mean that they believe that Covid-19 and all of its mutating progeny are Influenza Like Illnesses (ILIs). That’s because their assertion has bound Covid-19 activity (CLI) and the ILI category together. I share that perspective, but their charts and all of their public positions diverged from that path and created a cascade failure of confidence. To restore, consider that health scientists used to assert via the RSR, that broad spectrum antigenic and supporting tests under a transparent network of State and Federal laboratories and sentinels, provide the most accurate means to ground truth the circulating SRVs every year. The antigen tests are equally necessary to demonstrate the efficacy of therapeutics and vaccines. The CDC doesn’t have the option to turn these tests or the RSR on or off as it suits them.
This post has demonstrated a low key and partial nominal return by the CDC to RSR – like practices. That’s not nearly enough. The CDC and its SRV surveillance partners have never been granted a public license to break their own rules. And while respiratory virus test results for the sick appear to be anomalous if not defective, the health science communities which disregard, continue to pressure all others to test and pass continuously. This goes for their related pressures for all to take untested vaccines or even therapeutics to some extent.
Only an antigenic validation, such as the use of ferret – challenge studies can confirm which members of the vaccine study populations are ill with the target virus, and which are not. But according to the papers I’ve described in that link, antigenic animal challenge exercises do not appear to be included in the published vaccine studies for Covid-19 or any of its mutating progeny. Because this test information along with the most important verifications thereof, are important both to health and earth sciences, I’m committed to seeing that the CDC’s RSR is restored, and also that the past missing year is re-populated with the most transparent and accurate SRV data interpretations that can be found.
Includes opinions
References
 23513total visits,2visits today
23513total visits,2visits today